Course and Project Descriptions
BHLTH 420: Women's Global Health & Human Rights
This course is an advanced elective that provides students with the opportunity to apply multiple conceptual frameworks (e.g. human rights, social ecology of health model, and transnational feminism) to deconstruct factors that impact women’s* global health and human rights. During the term, we explore critical women's health issues from a lifespan perspective and across the world. We will read and listen to women’s lived experiences, review current research and scholarly evidence, examine international and domestic policy, dialogue about critical issues, and complete a Photovoice project with students on the West Bank in Palestine. We discuss difficult issues each week, but we will also examine examples of resistance and resilience, spotlight organizations and individuals who are creating change, and consider ways in which we can apply what we are discussing to our own professional practice and personal lives.
The course is particularly concerned with exploring non-Western views of women’s health and human rights issues. Particular attention will be paid to women from poorly resourced or developing areas of the world and on social ecological factors that impact vulnerability, marginalization, and population health. *Note: In this course, "women" refers to individuals who self-identify as such.
Purpose of the Project The primary objectives of this Photovoice project were as follows: 1) to learn and apply a participatory, community-engaged methodology (Photovoice) that allows pre-health professions students to improve their praxis; 2) to compare and contrast social ecological factors that impact the health and human rights of women in two different regions of the world; 3) to enhance students' ability to communicate and collaborate across cultures, time zones, and life circumstances; 4) to further interrogate the notion of "human rights" as a universal or primarily Western construct; 5) to better understand the challenges facing individuals (especially women) living in under military occupation; and 6) to raise social consciousness about global issues that influence wellness, social and political injustice; marginalization, and gender equity.
Methods: Students from the University of Washington Bothell collaborated with health professions students from Al Quds University in Hebron (West Bank) through a closed social media platform to learn the methods of Photovoice and to dialogue about concepts and issues shaping women's (trans and cis) global health and human rights. WA and West Bank students exchanged "photo stories" via a closed social media forum, through this website, and they shared their findings in a public exhibit on International Women's Day at the Northwest Film Forum, in Seattle, Washington.
The course is particularly concerned with exploring non-Western views of women’s health and human rights issues. Particular attention will be paid to women from poorly resourced or developing areas of the world and on social ecological factors that impact vulnerability, marginalization, and population health. *Note: In this course, "women" refers to individuals who self-identify as such.
Purpose of the Project The primary objectives of this Photovoice project were as follows: 1) to learn and apply a participatory, community-engaged methodology (Photovoice) that allows pre-health professions students to improve their praxis; 2) to compare and contrast social ecological factors that impact the health and human rights of women in two different regions of the world; 3) to enhance students' ability to communicate and collaborate across cultures, time zones, and life circumstances; 4) to further interrogate the notion of "human rights" as a universal or primarily Western construct; 5) to better understand the challenges facing individuals (especially women) living in under military occupation; and 6) to raise social consciousness about global issues that influence wellness, social and political injustice; marginalization, and gender equity.
Methods: Students from the University of Washington Bothell collaborated with health professions students from Al Quds University in Hebron (West Bank) through a closed social media platform to learn the methods of Photovoice and to dialogue about concepts and issues shaping women's (trans and cis) global health and human rights. WA and West Bank students exchanged "photo stories" via a closed social media forum, through this website, and they shared their findings in a public exhibit on International Women's Day at the Northwest Film Forum, in Seattle, Washington.

History of the Israeli-Palestinian Conflict
|
What is Photovoice?
Photovoice as a methodology involves much more than just handing people cameras and sending them out to take pictures or video. The participant (e.g. photographers) start by learning the basics of camera use and discussing safe and ethical documentary practices.In most cases, they meet regularly as a group (often jointly led by a photographer, researcher, and/or member of the group) to show and discuss the images they’ve taken, and to be able to state opinions and feelings in a safe and supportive environment. Other possible elements of a Photovoice project are discussed in the articles selected below. A Photovoice project or program can be an inexpensive and powerful tool for both life change and social change, but it needs to be planned and executed with a good deal of thought.
Since Photovoice is essentially a type of participatory action research, it can also be used in several ways: as a qualitative research method, as an assessment tool, as a way of gathering interpretive data, and as an evaluation tool. A Photovoice project can be freestanding, but is more often – and probably more effectively – run in collaboration with an existing group or coalition. There are a number of articles in scholarly peer reviewed journals that document the application of Photovoice towards conducting participatory needs assessment, asset-mapping, and evaluation. Seminal articles that provide a description and history of Photovoice. Wang, C. (2006). Youth participation in Photovoice as a strategy for community change. Journal of Community Practice. 14(1-2):147-161 Wang, C. et al. (1998). Photovoice as a participatory health promotion strategy. Health Promotion International. Case Studies Involving Photovoice in public and global health: Walker, A., and Oomen-Early, J. (2010). “We have to do something for ourselves": Using Photovoice and participatory action research with NGO workers to strengthen community capacity in Freetown, Sierra Leone. International Electronic Journal of Health Education, vol. 13, 33-48. Walker and Early Photovoice 2010 we have to do something for ourselves-1.pdf Wheeler, K. & Early, J. (2018). Using Photovoice to explore quality of life factors of adults with Crouzon Syndrome. Qualitative Health Research, vol(3):357-370. https://doi.org/10.1177/1049732317742624 |
Photos from the Public Event at Seattle's Northwest Film Forum
Amran Abdulahi, a Health Studies major at UW Bothell, discussed how gender equity impacts the health and well-being of women in the U.S. and Somalia.
|
UW Bothell student, MyKa'La Alexander, shared her photo story (not shown) and insights about the project with the audience.
|
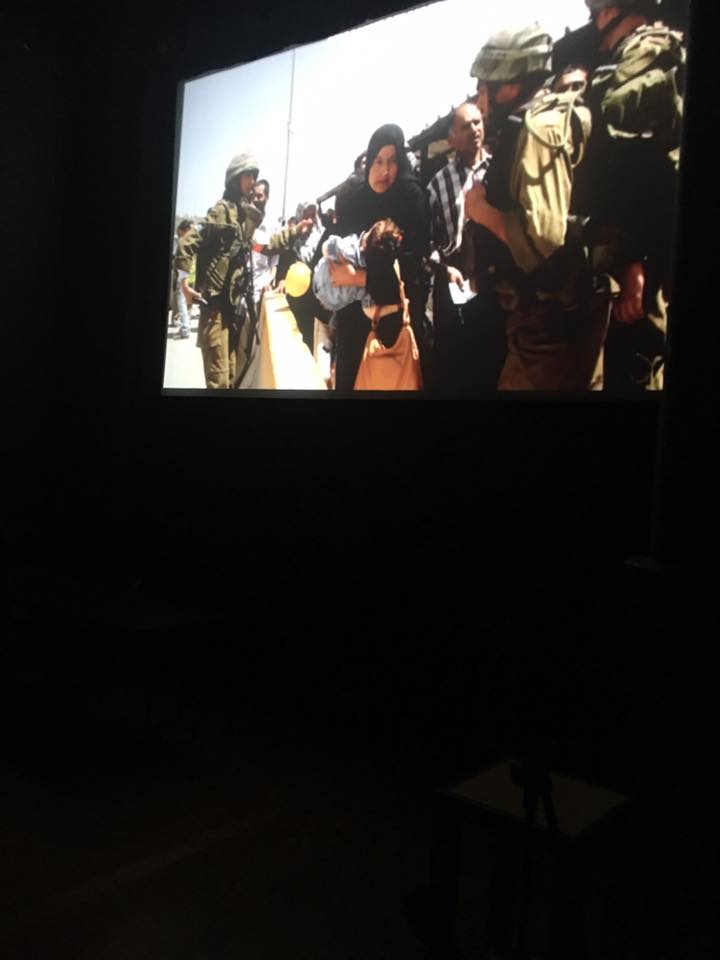
Although the students from Al Quds could not attend the event, their voices resonated through their video project which included interviews and images from women living in Hebron and Gaza, depicting life under occupation.
|
Visit the Washington State Dept. of Health to view reports on a number of health measures. http://www.doh.wa.gov/DataandStatisticalReports
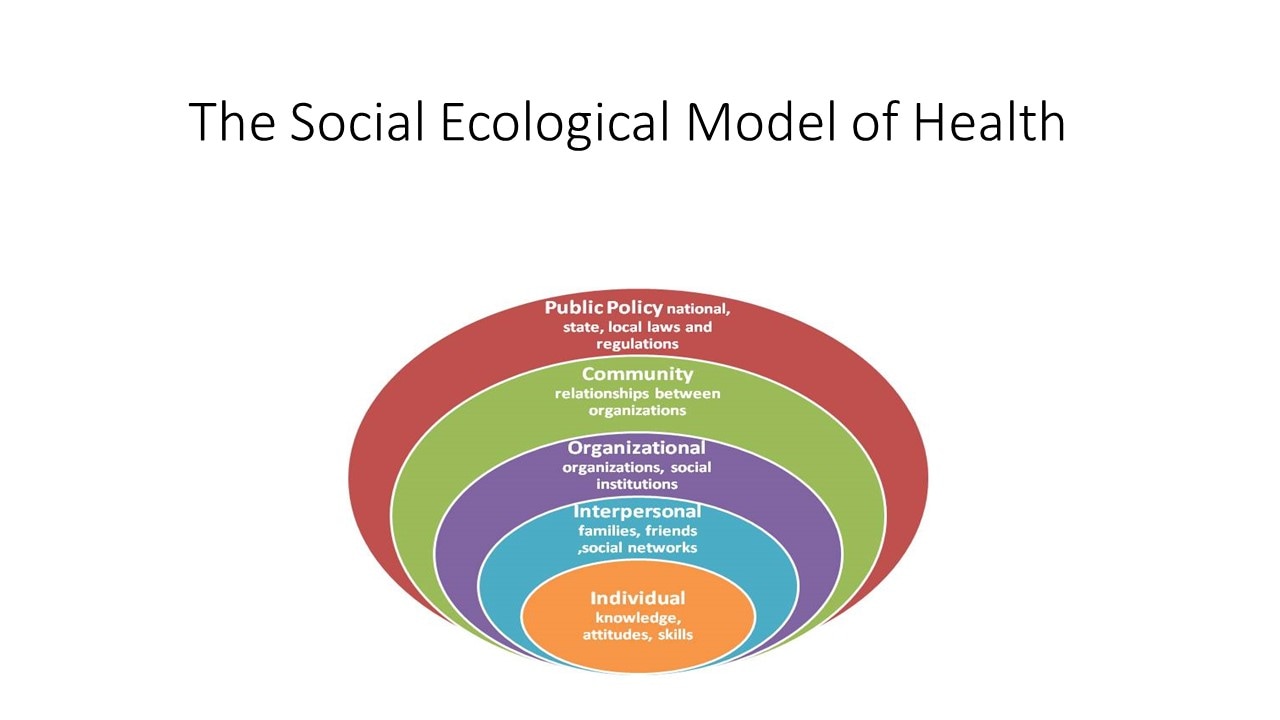
What is the Social Ecological Model of Health?
[Synopsis by Dr. Jody Early]
[Synopsis by Dr. Jody Early]
Modern health promotion involves more than simply educating individuals about healthy practices. It includes efforts to change organizational behavior, as well as understanding cultural and social norms, and addressing the the physical, social and environment of communities. It is also about developing and advocating for policies that support health, such as economic incentives. Health promotion programs that seek to address health problems across this spectrum employ a range of strategies, and operate on multiple levels.
The socio-ecological perspective emphasizes the interaction between, and interdependence of, factors within and across all levels of a health problem. It highlights people’s interactions with their physical and sociocultural environments. Two key concepts of the socio-ecological perspective help to identify intervention points for promoting health: first, behavior both affects, and is affected by, multiple levels of influence; second, individual behavior both shapes, and is shaped by, the social environment ( known as reciprocal causation).
To explain the first key concept of the socio-ecological perspective, multiple levels of influence, Dahlberg and Krug (2002) identified five levels of influence for healthrelated behaviors and conditions. Defined in Figure 1 (below) these levels include: (1) intrapersonal or individual factors; (2) interpersonal (relationship) factors; (3) institutional or organizational factors; (4) community factors; and (5) public policy factors (shown below).
In practice, addressing the community level requires taking into consideration institutional and public policy factors, as well as social networks and norms. Different levels of influence combine to affect population health. Each level of influence can affect health behavior.
Example: Women and Breast Cancer Screening
Suppose a woman over 50 delays getting a recommended mammogram (screening for breast cancer).
At the individual level, her inaction may be due to fears of finding out she has cancer. At the interpersonal level, her doctor may neglect to tell her that she should get the test, or she may have friends who say they do not believe it is important to get a mammogram. At the organizational level, it may be hard to schedule an appointment, because there is only a part-time radiologist at the clinic. At the policy level, she may lack insurance coverage, and thus be unable to afford the fee. Thus, the outcome, the woman’s failure to get a mammogram, may result from multiple factors.
The socio-ecological perspective emphasizes the interaction between, and interdependence of, factors within and across all levels of a health problem. It highlights people’s interactions with their physical and sociocultural environments. Two key concepts of the socio-ecological perspective help to identify intervention points for promoting health: first, behavior both affects, and is affected by, multiple levels of influence; second, individual behavior both shapes, and is shaped by, the social environment ( known as reciprocal causation).
To explain the first key concept of the socio-ecological perspective, multiple levels of influence, Dahlberg and Krug (2002) identified five levels of influence for healthrelated behaviors and conditions. Defined in Figure 1 (below) these levels include: (1) intrapersonal or individual factors; (2) interpersonal (relationship) factors; (3) institutional or organizational factors; (4) community factors; and (5) public policy factors (shown below).
In practice, addressing the community level requires taking into consideration institutional and public policy factors, as well as social networks and norms. Different levels of influence combine to affect population health. Each level of influence can affect health behavior.
Example: Women and Breast Cancer Screening
Suppose a woman over 50 delays getting a recommended mammogram (screening for breast cancer).
At the individual level, her inaction may be due to fears of finding out she has cancer. At the interpersonal level, her doctor may neglect to tell her that she should get the test, or she may have friends who say they do not believe it is important to get a mammogram. At the organizational level, it may be hard to schedule an appointment, because there is only a part-time radiologist at the clinic. At the policy level, she may lack insurance coverage, and thus be unable to afford the fee. Thus, the outcome, the woman’s failure to get a mammogram, may result from multiple factors.
Public Exhibit